 The 2019–20 coronavirus pandemic is an ongoing pandemic of coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). The outbreak was identified in Wuhan, China, in December 2019, declared to be a Public Health Emergency of International Concern on 30 January 2020, and recognized as a pandemic by the World Health Organization on 11 March 2020. As of 16 April 2020, more than 2.06 million cases of COVID-19 have been reported in 210 countries and territories, resulting in more than 137,000 deaths. More than 517,000 people have recovered, although there may be a possibility of relapse or reinfection. The deaths per diagnosed cases varies significantly between countries.
The 2019–20 coronavirus pandemic is an ongoing pandemic of coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). The outbreak was identified in Wuhan, China, in December 2019, declared to be a Public Health Emergency of International Concern on 30 January 2020, and recognized as a pandemic by the World Health Organization on 11 March 2020. As of 16 April 2020, more than 2.06 million cases of COVID-19 have been reported in 210 countries and territories, resulting in more than 137,000 deaths. More than 517,000 people have recovered, although there may be a possibility of relapse or reinfection. The deaths per diagnosed cases varies significantly between countries.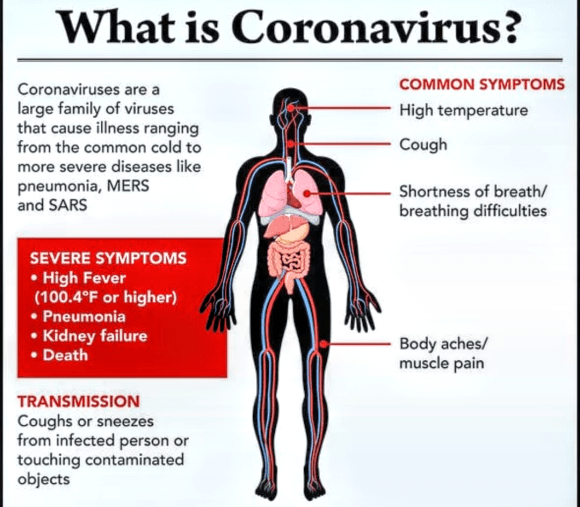
The virus is primarily spread between people during close contact, often via small droplets produced by coughing, sneezing, or talking. While these droplets are produced when breathing out, they usually fall to the ground or onto surfaces rather than being infectious over long distances. People may also become infected by touching a contaminated surface and then their face. The virus can survive on surfaces for up to 72 hours. It is most contagious during the first three days after the onset of symptoms, although spread may be possible before symptoms appear and in later stages of the disease. Common symptoms include fever, cough and shortness of breath. Complications may include pneumonia and acute respiratory distress syndrome. The time from exposure to onset of symptoms is typically around five days, but may range from two to fourteen days. There is no known vaccine or specific antiviral treatment. Primary treatment is symptomatic and supportive therapy.
Recommended preventive measures include hand washing, covering one’s mouth when coughing, maintaining distance from other people, and monitoring and self-isolation for people who suspect they are infected. Authorities worldwide have responded by implementing travel restrictions, quarantines, curfews and stay-at-home orders, workplace hazard controls, and facility closures.
The pandemic has led to severe global socioeconomic disruption, the postponement or cancellation of sporting, religious, political and cultural events, and widespread shortages of supplies exacerbated by panic buying. Schools, universities and colleges have closed either on a nationwide or local basis in 197 countries, affecting approximately 99.9 per cent of the world’s student population. Misinformation about the virus has spread online, and there have been incidents of xenophobia and discrimination against Chinese people and against those perceived as being Chinese or as being from areas with high infection rates. Due to reduced travel and closures of heavy industry, there has been a decrease in air pollution and carbon emissions.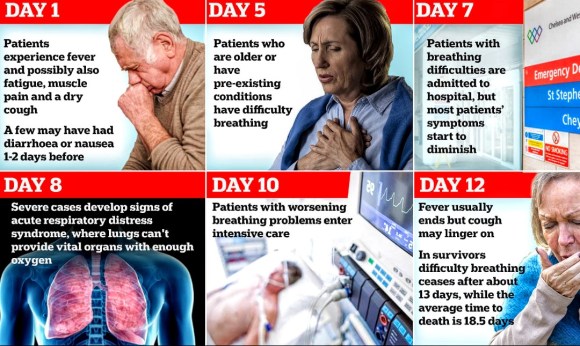
Health authorities in Wuhan, China (the capital of Hubei province), reported a cluster of pneumonia cases of unknown cause on 31 December 2019, and an investigation was launched in early January 2020. The cases mostly had links to the Huanan Seafood Wholesale Market and so the virus is thought to have a zoonotic origin. The virus that caused the outbreak is known as SARS-CoV-2, a newly discovered virus closely related to bat coronaviruses, pangolin coronaviruses, and SARS-CoV.
On 17 March 2020, scientists reported that virus originated naturally.
The earliest known person with symptoms was later discovered to have fallen ill on 1 December 2019, and that person did not have visible connections with the later wet market cluster. Of the early cluster of cases reported in December 2019, two-thirds were found to have a link with the market. On 13 March 2020, an unverified report from the South China Morning Post suggested a case traced back to 17 November 2019, in a 55-year-old from Hubei province, may have been the first.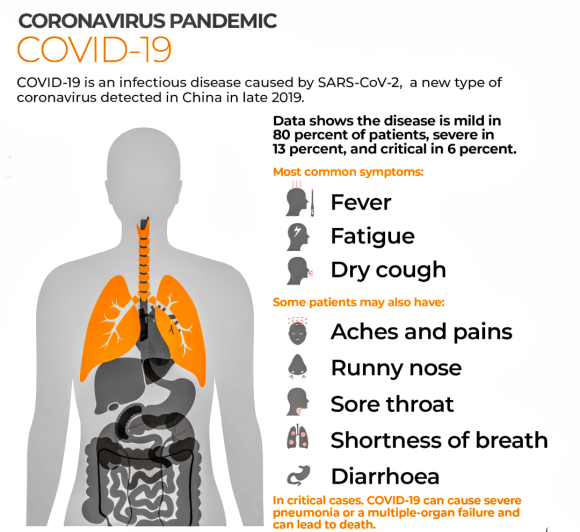
Cases
Cases refers to the number of people who have been tested for COVID-19, and whose test has been confirmed positive according to official protocols. As of 16 April, the countries that made public their testing data have on average tested only 1 per cent of their population, while no country has tested more than 10 per cent of its population. Many countries have had official policies not to test those with only mild symptoms, such as Italy, the Netherlands, Spain, and Switzerland. An analysis of the early phase of the outbreak up to 23 January estimated 86 per cent of COVID-19 infections had not been detected, and that these undocumented infections were the infection source for 79 per cent of documented cases. Several other studies, using a variety of methods, have estimated that numbers of infections in many countries are likely to be considerably greater than the reported cases. On 9 April 2020, preliminary results of testing showed that 15 per cent of people tested in Gangelt, the centre of a major infection cluster in Germany, had apparent immunity to SARS-COV-2.
Analysis by age in China indicates that a relatively low proportion of cases occur in individuals under 20 years of age. However, it is not yet clear whether this is because young people are actually less likely to be infected, or less likely to develop serious symptoms, and thus seek medical attention and be tested.
Initial estimates of the basic reproduction number (R0) for COVID-19 in January were between 1.4 and 2.5, buta subsequent statistical analysis has concluded that it may be much higher (between 3.8 and 8.9).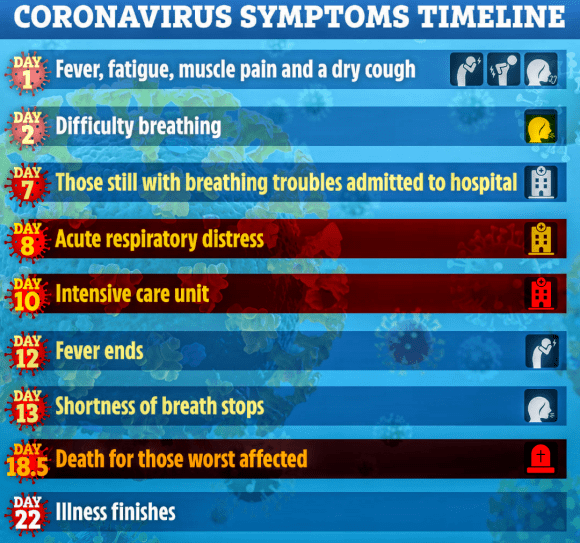
Deaths
Most people with COVID-19 recover. For those who do not, the time from development of symptoms to death has been between 6 and 41 days, with the most common being 14 days. As of 16 April 2020, approximately 137,000 deaths had been attributed to COVID-19. In China, as of 5 February about 80 per cent of deaths were in those over 60, and 75 per cent had pre-existing health conditions including cardiovascular diseases and diabetes.
The first confirmed death was in Wuhan on 9 January 2020. The first death outside mainland China occurred on 1 February in the Philippines, and the first death outside Asia was in France on 14 February. By 28 February, outside mainland China, more than a dozen deaths each were recorded in Iran, South Korea, and Italy. By 13 March, more than forty countries and territories had reported deaths, on every continent except Antarctica.
Official tallies of deaths from the COVID-19 pandemic generally refer to dead people who tested positive for COVID-19 according to official protocols. The number of true fatalities from COVID-19 may be much higher, as it may not include people who die without testing – e.g. at home or in nursing homes. There are indications of undercounting of deaths in Brazil, China,, Iran North Korea, Russia, the UK, andthe U.S.
Several measures are commonly used to quantify mortality. These numbers vary by region and over time, and are influenced by the volume of testing, healthcare system quality, treatment options, time since initial outbreak, and population characteristics such as age, sex, and overall health.
The death-to-case ratio reflects the number of deaths divided by the number of diagnosed cases within a given time interval. Based on Johns Hopkins University statistics, the global death-to-case ratio is 6.6 per cent (137,193 deaths for 2,069,819 cases) as of 16 April 2020. The number varies by region. In China, estimates for the death-to-case ratio decreased from 17.3 per cent (for those with onset of symptoms from 1 to 10 January 2020) to 0.7 per cent (for those with onset of symptoms after 1 February 2020).
Other measures include the case fatality rate (CFR), which reflects the percentage of diagnosed people who die from a disease, and the infection fatality rate (IFR), which reflects the percentage of infected (diagnosed and undiagnosed) who die from a disease. These statistics are not timebound and follow a specific population from infection through case resolution. The University of Oxford’s Centre for Evidence-Based Medicine maintains an ongoing review of both CFR and IFR estimates, and as of 9 April they estimated a CFR of 0.72 per cent, but they also caution that there is considerable uncertainty at this stage in the pandemic.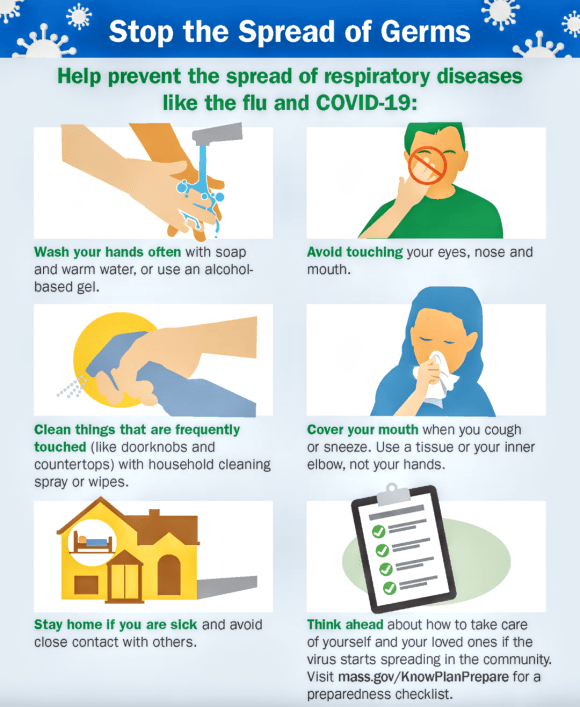
Duration
The WHO asserts that the pandemic can be controlled. The peak and ultimate duration of the outbreak are uncertain and may differ by location. Maciej Boni of Penn State University stated, “Left unchecked, infectious outbreaks typically plateau and then start to decline when the disease runs out of available hosts. But it’s almost impossible to make any sensible projection right now about when that will be”. The Chinese government’s senior medical adviser Zhong Nanshan argued that “it could be over by June” if all countries can be mobilized to follow the WHO’s advice on measures to stop the spread of the virus. On 17 March, Adam Kucharski of the London School of Hygiene & Tropical Medicine said SARS-CoV-2 “is going to be circulating, potentially for a year or two”. According to the Imperial College study led by Neil Ferguson, physical distancing and other measures will be required “until a vaccine becomes available (potentially 18 months or more)”. William Schaffner of Vanderbilt University stated, “I think it’s unlikely that this coronavirus – because it’s so readily transmissible – will disappear completely” and it “might turn into a seasonal disease, making a comeback every year”. The virulence of the comeback would depend on herd immunity and the extent of mutation.
Signs and symptoms

Symptoms of COVID-19 can be relatively non-specific and infected people may be asymptomatic. The two most common symptoms are fever (88 per cent) and dry cough (68 per cent). Less common symptoms include fatigue, respiratory sputum production (phlegm), loss of the sense of smell, shortness of breath, muscle and joint pain, sore throat, headache, chills, vomiting, hemoptysis, diarrhoea, or cyanosis.
The WHO says approximately one person in five becomes seriously ill and has difficulty breathing. The U.S. Centers for Disease Control and Prevention (CDC) lists emergency symptoms as difficulty breathing, persistent chest pain or pressure, sudden confusion, difficulty waking, and bluish face or lips; immediate medical attention is advised if these symptoms are present.
Further development of the disease can lead to severe pneumonia, acute respiratory distress syndrome, sepsis, septic shock and death. Some of those infected may be asymptomatic, with no clinical symptoms but with test results that confirm infection, so researchers have issued advice that those with close contact to confirmed infected people should be closely monitored and examined to rule out infection. Chinese estimates of the asymptomatic ratio range from few to 44 per cent. The usual incubation period (the time between infection and symptom onset) ranges from one to 14 days; it is most commonly five days.
As an example of uncertainty, the estimate of the fraction of people with COVID-19 who lost their sense of smell was initially 30 per cent but later fell to 15 per cent.
Transmission
Some details about how the disease is spread are still being determined. The disease is believed to be primarily spread during close contact and by small droplets produced during coughing, sneezing, or talking; with close contact being within 1 to 2 metres (3 to 6 feet). Both sputum and saliva can carry large viral loads. Studies have found that an uncovered cough can lead to droplets travelling up to 4.5 metres (15 feet) to 11.4 metres (37 feet). Some have proposed that the virus may also be transmitted by small droplets that stay for more prolonged periods in the air, as may be generated during speech.
Respiratory droplets may also be produced during breathing out, including when talking, though the virus is not generally airborne. The droplets can land in the mouths or noses of people who are nearby or possibly be inhaled into the lungs. Some medical procedures such as intubation and cardiopulmonary resuscitation (CPR) may cause respiratory secretions to be aerosolized and thus result in airborne spread. It may also spread when one touches a contaminated surface, including skin, and then touches their eyes, nose, or mouth. While there are concerns it may spread by faeces, this risk is believed to be low. The Government of China denied the possibility of faecal–oral transmission of SARS-CoV-2.
The virus is most contagious during the first three days after onset of symptoms, although spread may be possible before symptoms appear and in later stages of the disease. People have tested positive for the disease up to three days before onset of symptoms suggesting transmission is possible before developing significant symptoms. Only few reports of laboratory-confirmed asymptomatic cases exist, but asymptomatic transmission has been identified by some countries during contact tracing investigations. The European Centre for Disease Prevention and Control (ECDC) says that while it is not entirely clear how easily the disease spreads, one person generally infects two to three others.
The virus survives for hours to days on surfaces. Specifically, the virus was found to be detectable for up to three days on plastic (polypropylene) and 304 stainless steel, for one day on cardboard, and for up to four hours on copper. This, however, varies based on the humidity and temperature.
Pets and other animals have tested positive for COVID-19. There is no evidence animals can pass the virus on to humans, though British authorities advise washing one’s hands after contact with animals, like after contact with other potentially contaminated surfaces.
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is a novel virus, first isolated from three people with pneumonia connected to the cluster of acute respiratory illness cases in Wuhan. All features of the novel SARS-CoV-2 virus occur in related coronaviruses in nature.
Outside the human body, the virus is killed by household soap, which dissolves its protective envelope.
SARS-CoV-2 is closely related to SARS-CoV, and is thought to have a zoonotic origin. Genetic analysis has revealed that SARS-CoV-2 genetically clusters with the genus Betacoronavirus, in subgenus Sarbecovirus (lineage B) together with two bat-derived strains. It is 96 per cent identical at the whole genome level to other bat coronavirus sample and 92 per cent identical to pangolin coronavirus. It is unclear which animal was the intermediate host.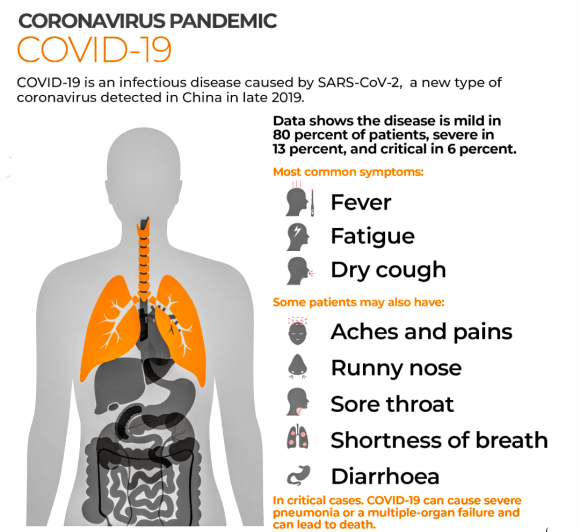
Diagnosis
Infection by the virus can be provisionally diagnosed on the basis of symptoms, though confirmation is ultimately by reverse transcription polymerase chain reaction (rRT-PCR) of infected secretions or CT imaging. A study comparing PCR to CT in Wuhan has suggested that CT is significantly more sensitive than PCR, though less specific, with many of its imaging features overlapping with other pneumonias and disease processes. As of March 2020, the American College of Radiology recommends that “CT should not be used to screen for or as a first-line test to diagnose COVID-19”.
Viral testing
The WHO has published several RNA testing protocols for SARS-CoV-2, with the first issued on 17 January. The test uses real-time reverse transcription polymerase chain reaction (rRT-PCR). The test can be done on respiratory or blood samples. Results are generally available within a few hours to days. Generally this test is carried out on a nasopharyngeal swab though a throat swab may also be used.
A number of laboratories and companies are developing serological tests, which detect antibodies. As of 6 April 2020, none of these has been proved sufficiently accurate to be approved for widespread use. In the U.S. a serological test developed by Cellex has been approved for emergency use by certified laboratories only.
Characteristic imaging features on radiographs and computed tomography (CT) of people who are symptomatic include asymmetric peripheral ground glass opacities and absent pleural effusions. The Italian Radiological Society is compiling an international online database of imaging findings for confirmed cases. Due to overlap with other infections such as adenovirus, imaging without confirmation by PCR is of limited specificity in identifying COVID-19. A large study in China compared chest CT results to PCR and demonstrated that though imaging is less specific for the infection, it is faster and more sensitive, suggesting its consideration as a screening tool in epidemic areas. Artificial intelligence-based convolutional neural networks have been developed to detect imaging features of the virus with both radiographs and CT.
Prevention
Strategies for preventing transmission of the disease include maintaining overall good personal hygiene, washing hands, avoiding touching the eyes, nose, or mouth with unwashed hands, and coughing or sneezing into a tissue and putting the tissue directly into a waste container. Those who may already have the infection have been advised to wear a surgical mask in public. Physical distancing measures are also recommended to prevent transmission. Health care providers taking care of someone who may be infected are recommended to use standard precautions, contact precautions, and eye protection.
Many governments have restricted or advised against all non-essential travel to and from countries and areas affected by the outbreak. However, the virus is already spreading within communities in large parts of the world, with many not knowing where or how they were infected.
Contact tracing is an important method for health authorities to determine the source of an infection and to prevent further transmission. Theuse of location data from mobile phones by governments for this purpose has prompted privacy concerns, with Amnesty International and more than a hundred other organizations issuing a statement calling for limits on this kind of surveillance.
Various mobile apps have been implemented or proposed for voluntary use, and as of 7 April 2020 more than a dozen expert groups were working on privacy-friendly solutions such as using Bluetooth to log a user’s proximity to other cellphones. Users could then receive a message if they’ve been in close contact with someone who has subsequently tested positive for COVID-19.
On 10 April 2020 Google and Apple, jointly announced an initiative for privacy-preserving contact tracing based on Bluetooth technology and cryptography. The system is intended to allow governments to create official privacy-preserving coronavirus tracking apps, with the eventual goal of integration of this functionality directly into the iOS and Android mobile platforms.
Misconceptions are circulating about how to prevent infection; for example, rinsing the nose and gargling with mouthwash are not effective. There is no COVID-19 vaccine, though many organizations are working to develop one.
Hand washing
Hand washing is recommended to prevent the spread of the disease. The CDC recommends that people wash hands often with soap and water for at least twenty seconds, especially after going to the toilet or when hands are visibly dirty; before eating; and after blowing one’s nose, coughing, or sneezing. This is because outside the human body, the virus is killed by household soap, which bursts its protective bubble. CDC further recommended using an alcohol-based hand sanitizer with at least 60 per cent alcohol by volume when soap and water are not readily available. The WHO advises people to avoid touching the eyes, nose, or mouth with unwashed hands.
Surface cleaning
Surfaces may be decontaminated with a number of solutions (within one minute of exposure to the disinfectant for a stainless steel surface), including 62–71 per cent ethanol, 50–100 per cent isopropanol, 0.1 per cent sodium hypochlorite, 0.5 per cent hydrogen peroxide, and 0.2–7.5 per cent povidone-iodine. Other solutions, such as benzalkonium chloride and chrohexidine gluconate, are less effective. The CDC recommends that if a COVID case is suspected or confirmed at a facility such as an office or day care, all areas such as offices, bathrooms, common areas, shared electronic equipment like tablets, touch screens, keyboards, remote controls, and ATM machines used by the ill persons, should be disinfected.
Face masks and respiratory hygiene
Masks have also been recommended for use by those taking care of someone who may have the disease. The WHO has recommended the wearing of masks by healthy people only if they are at high risk, such as those who are caring for a person with COVID-19, although they also acknowledge that wearing masks may help people avoid touching their face. Multiple countries encourage the use of face masks more generally by members of the public, several of them making wearing masks obligatory.
Social distancing
Social distancing (also known as physical distancing) includes infection control actions intended to slow the spread of disease by minimizing close contact between individuals. Methods include quarantines; travel restrictions; and the closing of schools, workplaces, stadiums, theatres, or shopping centres. Individuals may apply social distancing methods by staying at home, limiting travel, avoiding crowded areas, using no-contact greetings, and physically distancing themselves from others. Many government are now mandating or recommending social distancing in regions affected by the outbreak. The maximum gathering size recommended by U.S. government bodies and health organizations was swiftly reduced from 250 people (if there was no known COVID-19 spread in a region) to 50 people, and later to 10 people. On 22 March 2020, Germany banned public gatherings of more than two people. A Cochrane review found that early quarantine with other public health measures are effective in limiting the pandemic, but the best manner of adopting and relaxing policies are uncertain, as local conditions vary.
The pandemic in Peru resulted with enforced curfews by the Peruvian Armed Forces.
Older adults and those with underlying medical conditions such as diabetes, heart disease, respiratory disease, hypertension, and compromised immune systems face increased risk of serious illness and complications and have been advised by the CDC to stay home as much as possible in areas of community outbreak.
In late March 2020, the WHO and other health bodies began to replace the use of the term “social distancing” with “physical distancing”, to clarify that the aim is to reduce physical contact while maintaining social connections, either virtually or at a distance. The use of the term “social distancing” had led to implications that people should engage in complete social isolation, rather than encouraging them to stay in contact with others through alternative means.
Some authorities have issued sexual health guidelines for use during the pandemic. These include recommendations to have sex only with someone you live with, and who does not have the virus or symptoms of the virus.
Self-isolation
Self-isolation at home has been recommended for those diagnosed with COVID-19 and those who suspect they have been infected. Health agencies have issued detailed instructions for proper self-isolation.
Many governments have mandated or recommended self-quarantine for entire populations living in affected areas. The strongest self-quarantine instructions have been issued to those in high risk groups. Those who may have been exposed to someone with COVID-19 and those who have recently travelled to a country or region with widespread transmission have been advised to self-quarantine for 14 days from the time of last possible exposure.
Strategies in the control of an outbreak are containment or suppression, and mitigation. Containment is undertaken in the early stages of the outbreak and aims to trace and isolate those infected as well as introduce other measures of infection control and vaccinations to stop the disease from spreading to the rest of the population. When it is no longer possible to contain the spread of the disease, efforts then move to the mitigation stage: measures are taken to slow the spread and mitigate its effects on the healthcare system and society. A combination of both containment and mitigation measures may be undertaken at the same time. Suppression requires more extreme measures so as to reverse the pandemic by reducing the basic reproduction number to less than 1.
Part of managing an infectious disease outbreak is trying to decrease the epidemic peak, known as flattening the epidemic curve. This decreases the risk of health services being overwhelmed and provides more time for vaccines and treatments to be developed. Non-pharmaceutical interventions that may manage the outbreak include personal preventive measures, such as hand hygiene, wearing face-masks, and self-quarantine; community measures aimed at physical distancing such as closing schools and cancelling mass gathering events; community engagement to encourage acceptance and participation in such interventions; as well as environmental measures such surface cleaning.
Semi-log graph of new cases and deaths in China during Covid-19 epidemic showing the lockdown and lifting More drastic actions aimed at containing the outbreak were taken in China once the severity of the outbreak became apparent, such as quarantining entire cities and imposing strict travel bans.
Simulations for Great Britain and the United States show that mitigation (slowing but not stopping epidemic spread) and suppression (reversing epidemic growth) have major challenges. Optimal mitigation policies might reduce peak healthcare demand by 2/3 and deaths by half, but still result in hundreds of thousands of deaths and health systems being overwhelmed. Suppression can be preferred but needs to be maintained for as long as the virus is circulating in the human population (or until a vaccine becomes available), as transmission otherwise quickly rebounds when measures are relaxed. Long-term intervention to suppress the pandemic causes social and economic costs.
| Disease | Coronavirus disease 2019 (COVID-19) |
|---|---|
| Virus strain | Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) |
| Source | Bats or possibly pangolins |
| Location | Worldwide (list of locations) |
| Index case | Wuhan, Hubei, China 30°37′11″N 114°15′28″E |
| Date | December 2019 – present (4 months and 2 weeks) |
| Confirmed cases | 2,069,819 |
| Recovered | 517,931 |
|
Deaths
|
137,193 |
|
Territories
|
210 |
Articles By Wikipedia
